


Alcohol, Brain Health, and Longevity
Placing the good, the bad, and the uncertain, into context
décembre 31, 2025

I love a glass of wine with dinner, having grown up in an Italian origin family, so this article pains me a little to write. The new studies pretty clearly point to even low levels of alcohol being harmful, but the magnitude of harm is on the lower side relatively speaking, at least for most people, and there are still some open questions. The news headlines about how harmful alcohol is have led to people drinking less in my circles and life becoming a little less fun in my opinion. A dry party is often more button-upped, where people don’t open up or connect as deeply, and go home early. Boo.
This Substack is reader-supported. To receive new posts and support my work, consider becoming a free or paid subscriber.Subscribe
Health is a series of tradeoffs. Hopefully this article will put any alcohol tradeoffs that you are contemplating into deeper context.
I also hope that someone will create a better version of alcohol with all the positives and none of the harms because I do think we need some pharmacological help connecting, at least in this day and age with the ongoing post-COVID era “loneliness epidemic”.
Why the all the news headlines about the harms of alcohol?
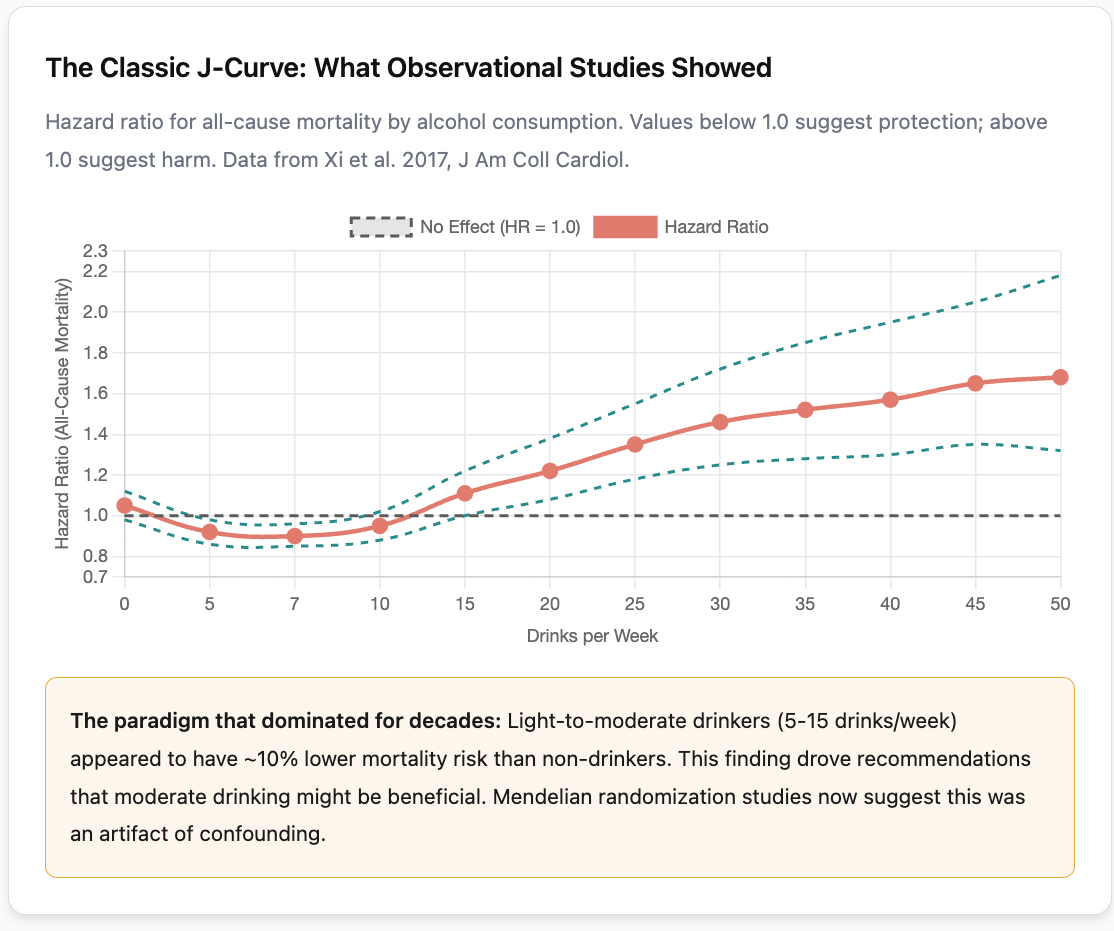
For years, you may have heard that a glass of wine with dinner is good for your brain, or that moderate drinkers live longer than teetotalers. These ideas were based on decades of observational research showing what scientists call a “J-shaped curve,” where light drinkers appeared healthier than both non-drinkers and heavy drinkers.
Recent research using genetic methods has complicated this picture. The largest Mendelian randomization studies from 2024 and 2025, including Topiwala et al., analyzing data from over 2 million people, suggest that alcohol’s apparent protective effects may be an artifact of how earlier studies were designed rather than a real biological benefit. But the evidence is more nuanced than headlines suggest: earlier genetic studies found no association in either direction, and important questions remain about effects at very low consumption levels, in different populations, and across the lifespan.
Here I dive into the evidence, including the neuropharmacology that explains why alcohol feels good and why it persists across cultures, how Mendelian randomization works and why it produces different results than observational studies; the critical limitations of MR, particularly horizontal pleiotropy (when “alcohol genes” also predict impulsivity, risk-taking, and psychiatric conditions), why randomized controlled trials haven’t been done, including the scandal that derailed the only serious attempt (the MACH trial), the cancer risks that MR has helped clarify (with absolute risk calculations), how APOE4 genetic status may modify alcohol’s effects, the social benefits we might lose if we eliminate drinking, and what alternatives might fill that void.
What we can say with reasonable confidence is that the old narrative of “moderate drinking is good for your brain” is not supported by the best current evidence. What remains genuinely uncertain is whether light drinking causes meaningful harm, has negligible effects, or might even provide small benefits in specific contexts that we don’t yet understand.
Why alcohol feels good: the neuropharmacology of a drink
Before examining alcohol’s risks, it helps to understand why humans have consumed it for millennia and why it remains so deeply embedded in social life. Alcohol is not simply a toxin people tolerate for cultural reasons; it produces genuine neurological effects that many find pleasurable and useful.
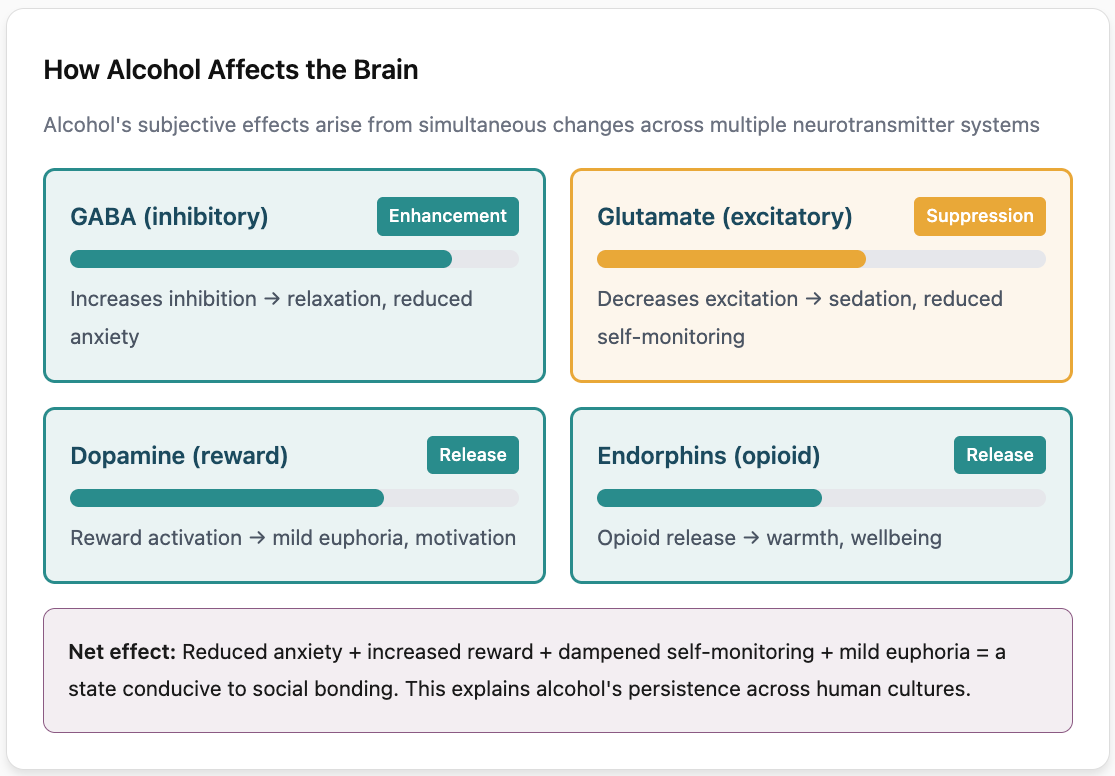
GABA enhancement and anxiety reduction. Alcohol’s primary mechanism is enhancing the effect of gamma-aminobutyric acid (GABA), the brain’s main inhibitory neurotransmitter. When alcohol binds to GABA-A receptors, it increases chloride ion flow into neurons, making them less likely to fire. This dampens activity across much of the brain, producing the characteristic feeling of relaxation. For people with social anxiety or general nervousness, this effect can feel like relief: the internal chatter quiets, self-consciousness fades, and social interaction becomes easier. This is not imaginary or merely psychological; it reflects real changes in neural activity, particularly in the amygdala (the brain’s threat-detection center) and prefrontal cortex (involved in self-monitoring and worry).
Dopamine release and reward. Alcohol also triggers dopamine release in the nucleus accumbens, the brain’s reward center. This produces mild euphoria and reinforces the behavior of drinking.
Endorphin release. Alcohol stimulates the release of endogenous opioids (endorphins) in the brain, contributing to feelings of warmth and well-being. Brain imaging studies show that alcohol consumption increases endorphin release in the orbitofrontal cortex and nucleus accumbens, and that people who experience greater endorphin release report feeling more intoxicated. This opioid component may help explain alcohol’s pain-relieving properties and its particular appeal during emotional distress.
Glutamate suppression. Alcohol inhibits glutamate, the brain’s main excitatory neurotransmitter, by blocking NMDA receptors. This contributes to the sedative effects and memory impairment associated with higher doses. At lower doses, the combination of GABA enhancement and glutamate suppression produces a state of relaxed alertness that many find conducive to conversation and social bonding.
Why this matters for social function. The net effect of these mechanisms is a temporary shift in brain state: reduced anxiety, increased reward sensitivity, dampened self-monitoring, and mild euphoria. For social interaction, this combination can be genuinely useful. The prefrontal cortex normally maintains vigilance about how we are being perceived, generating self-conscious thoughts that can interfere with spontaneous connection. Alcohol quiets this monitoring, making it easier to speak freely, laugh, and feel present with others. The shared experience of this altered state, combined with cultural rituals around drinking, creates a context for bonding that many people find difficult to replicate otherwise.
This is not to say these effects are worth the costs. But understanding the pharmacology helps explain why alcohol has been so persistent across human cultures, why non-alcoholic beverages do not fully substitute for it, and why any serious attempt to reduce alcohol’s harms must grapple with providing alternative routes to these neurological states.
Understanding Mendelian randomization: using genetics to find true cause and effect
The most important methodological advance behind the shift in our understanding of alcohol’s harms is a technique called Mendelian randomization. To understand why it matters, consider the challenge researchers face: people who drink moderately are different from non-drinkers in many ways beyond their alcohol consumption. They tend to be wealthier, more socially connected, better educated, and healthier overall. When we observe that moderate drinkers have lower dementia rates, we cannot know whether alcohol is helping them or whether other aspects of their lives are responsible.
Mendelian randomization solves this problem by using genetics as a natural experiment. Certain genes affect how efficiently people metabolize alcohol, influencing how much people tend to drink over their lifetimes. By comparing dementia rates between people who are genetically predisposed to drink more versus less, researchers can isolate the effect of alcohol itself from confounding lifestyle factors. It is similar to a randomized controlled trial conducted by nature over a lifetime.
When researchers applied these methods to data from 2.4 million people across 45 studies, the protective effect of moderate drinking disappeared entirely. Instead, the largest studies found a straightforward linear relationship: more alcohol means higher dementia risk, starting from the first drink.
As lead researcher Dr. Anya Topiwala stated in the 2025 BMJ Evidence-Based Medicine study, “Genetic evidence offers no support for a protective effect; in fact, it suggests the opposite.”
The hidden confounds in MR: when “alcohol genes” predict more than drinking
Mendelian randomization is often presented as a way to eliminate confounding, but it has its own blind spots. One is population stratification: You may have heard of the “Asian flush” variant (ALDH2), which makes alcohol unpleasant for carriers and is common in East Asian populations but rare in Europeans. If researchers simply compared carriers to non-carriers across populations, they would be comparing groups that differ in many ways beyond alcohol metabolism: diet, lifestyle, healthcare systems, and thousands of other genetic variants. This would violate MR’s core assumption that the genetic instrument is independent of confounders.
The large MR studies cited here handle this in several ways. First, most restrict analyses to single ancestry groups, predominantly European, to avoid cross-population confounding. Second, rather than relying on single variants like ALDH2, they use polygenic scores combining 95 or more SNPs that affect alcohol consumption through various pathways. Third, they statistically control for population structure using principal components. These approaches reduce but do not eliminate concerns about population stratification, and they also mean findings may not generalize well across ancestries. Studies in East Asian populations using ALDH2 as an instrument have produced mixed results, with some finding associations and others finding none.
The second and most significant is horizontal pleiotropy, the possibility that the genetic variants used to instrument alcohol consumption also affect other traits that independently influence mortality or dementia. If this is happening, MR studies could show harm from “alcohol” when the true culprit is something else the genes predict.
This concern is not hypothetical. The genetic variants used in alcohol MR studies are not just metabolism genes like ADH1B and ALDH2. Modern studies use 94 or more SNPs identified from genome-wide association studies of drinking behavior. Many of these variants are associated with a constellation of traits beyond alcohol consumption:
- Impulsivity and sensation seeking: The gene CADM2, consistently associated with alcohol consumption in GWAS, is also linked to risk tolerance, automobile speeding, number of sexual partners, and cannabis use. People with genetic variants predisposing them to drink more may also be genetically predisposed to take more risks generally.
- Externalizing behaviors: Research shows that the majority of genetic variance for alcohol use disorder is shared with a broad “externalizing” factor that includes ADHD, conduct disorder, antisocial behavior, and general behavioral disinhibition. The genes may be tagging this latent liability rather than alcohol specifically.
- Psychiatric conditions: Alcohol-associated variants overlap substantially with those for depression, anxiety, and other psychiatric disorders. These conditions independently increase mortality risk.
- Smoking: Genetic variants at PDE4B and CUL3 are associated with both alcohol consumption and smoking behavior. Since smoking clearly increases mortality, any MR study using these variants as alcohol instruments will partially capture smoking effects.
MR studies attempt to address pleiotropy using sensitivity analyses like MR-Egger, weighted median, and MR-PRESSO, which can detect and adjust for some forms of horizontal pleiotropy. The Kassaw et al. 2024 study, for example, found consistent results across five different MR methods, which increases confidence that the findings are robust. But these methods assume that pleiotropic effects are either random or uncorrelated with the exposure effect. If the pleiotropy operates through a shared underlying factor, like a general tendency toward behavioral disinhibition, these corrections may not fully work.
Consider this thought experiment: Suppose there exists a genetic factor we might call “behavioral constraint” that influences how carefully people manage their lives. People with less genetic constraint drink more, smoke more, take more risks, exercise less, and manage chronic diseases less carefully. An MR study instrumenting alcohol with these genes would show that “genetically predicted alcohol” increases mortality, but the true cause would be the underlying behavioral pattern, not the alcohol itself.
The strongest evidence against this interpretation comes from the ADH1B and ALDH2 variants, which directly affect alcohol metabolism through well-understood biochemical pathways and have minimal association with other traits. Studies using only these variants also find harm from alcohol, though with less statistical power due to using fewer instruments. Additionally, the consistency of findings across different MR methods and populations provides some reassurance that pleiotropy is not fully explaining the results.
But we should maintain appropriate epistemic humility. MR is not a perfect randomized trial, it is a sophisticated statistical technique with assumptions that can be violated. The finding that “genetically predicted alcohol consumption” is associated with mortality is robust; the interpretation that alcohol itself causes that mortality, independent of the behavioral and psychiatric traits that travel with it, requires additional assumptions that may not hold perfectly.
Not all Mendelian randomization studies agree
It is important to note that earlier MR studies produced more ambiguous results. A 2020 study found no evidence of a causal association between alcohol consumption and late-onset Alzheimer’s disease risk, though it did find alcohol was associated with earlier age of onset. A 2024 study in the Health and Retirement Study similarly found null associations, concluding that “Mendelian randomization approaches show no association with alcohol and dementia.” A review of prior MR investigations noted that studies have “largely found null associations between alcohol use and cognitive impairment or dementia.”
Why might MR studies conflict? Several factors matter. First, sample size: earlier studies were smaller and may have been underpowered to detect modest effects. The 2025 studies drew on genetic data from 2.4 million participants, dwarfing previous analyses. Second, the outcome measured: some studies focused specifically on Alzheimer’s disease rather than all-cause dementia, and the relationship may differ by dementia subtype. Third, the genetic instruments used: earlier studies often relied on single SNPs in alcohol metabolism genes (like ALDH2 and ADH1B), while newer studies use polygenic scores based on 95 or more variants, providing stronger instruments. Fourth, the populations studied: MR assumptions may be violated differently across ancestries and age groups.
The most recent and largest MR studies consistently find linear harm, but the earlier null findings remind us that this is an evolving field. What we can say with confidence is that MR studies find either no effect or harm; none support the protective effects suggested by observational research.
Why we don’t have randomized trials: ethics, logistics, and the MACH scandal
The gold standard for establishing causality in medicine is the randomized controlled trial. If we could randomly assign thousands of people to drink moderately or abstain for a decade, then measure dementia and mortality rates, we would have a definitive answer. So why hasn’t this been done?
The barriers are formidable. First, ethics: Alcohol is a known carcinogen (classified as Group 1 by the International Agency for Research on Cancer, the same category as tobacco and asbestos). Randomly assigning people to consume a carcinogen for years raises serious ethical concerns, particularly when emerging evidence suggests harm even at low doses. An institutional review board would need to weigh whether the scientific value justifies the potential risk to participants.
Second, compliance: Unlike a pill that can be taken or not taken, alcohol consumption is deeply embedded in social life. Participants assigned to abstain might drink anyway, those assigned to drink might reduce consumption. Over a multi-year study, maintaining adherence to assigned drinking levels would be extremely difficult. This “crossover” between groups would dilute any true effect and potentially render the trial uninformative.
Third, duration and cost: Dementia and cardiovascular disease develop over decades. A trial powered to detect meaningful differences in these outcomes would need to follow thousands of participants for 6-10 years minimum, at enormous expense, likely $100 million or more.
Fourth, blinding: Participants obviously know whether they’re drinking alcohol or not, making true blinding impossible. This introduces potential for placebo effects and behavioral changes that could confound results.
Despite these challenges, one major trial was actually attempted. The Moderate Alcohol and Cardiovascular Health (MACH) trial aimed to randomize 7,800 participants to either one drink per day or no alcohol, following them for six years to assess cardiovascular disease and diabetes outcomes. Enrollment began in February 2018.
Three months later, the NIH terminated the trial. An investigation revealed that NIAAA officials had secretly courted the alcohol industry to fund the $100 million study, with money funneled through the NIH Foundation. Emails showed researchers telling alcohol executives that the trial “represents a unique opportunity to show that moderate alcohol consumption is safe and lowers risk of common diseases” and would provide “the level of evidence necessary if alcohol is to be recommended as part of a healthy diet.”
The NIH working group found that these interactions “appear to intentionally bias the framing of the scientific premise in the direction of demonstrating a beneficial health effect.” The trial design was also criticized for being underpowered to detect cancer harms. It would run long enough to potentially show cardiovascular benefits while missing the increased cancer risk that accumulates over longer timeframes. As the investigators concluded: “the trial could show benefits while missing the harms.”
The MACH scandal illustrates a broader problem: the alcohol industry has strong commercial interests in research showing health benefits, while there is no comparable commercial interest in demonstrating harm. This asymmetry has likely shaped the research landscape for decades, with industry-funded observational studies disproportionately finding benefits.
So we are left with imperfect tools. Observational studies are confounded. Mendelian randomization has its own assumptions and limitations. And the one serious attempt at a randomized trial was corrupted by industry influence before it could generate meaningful data. This is why the question of whether moderate alcohol consumption is truly harmful, or whether the harm shown in MR studies reflects pleiotropy, remains genuinely uncertain. We are doing our best to triangulate truth from flawed methods, each with different biases, hoping their errors don’t all point in the same direction.
How much alcohol affects dementia risk: putting the numbers in context
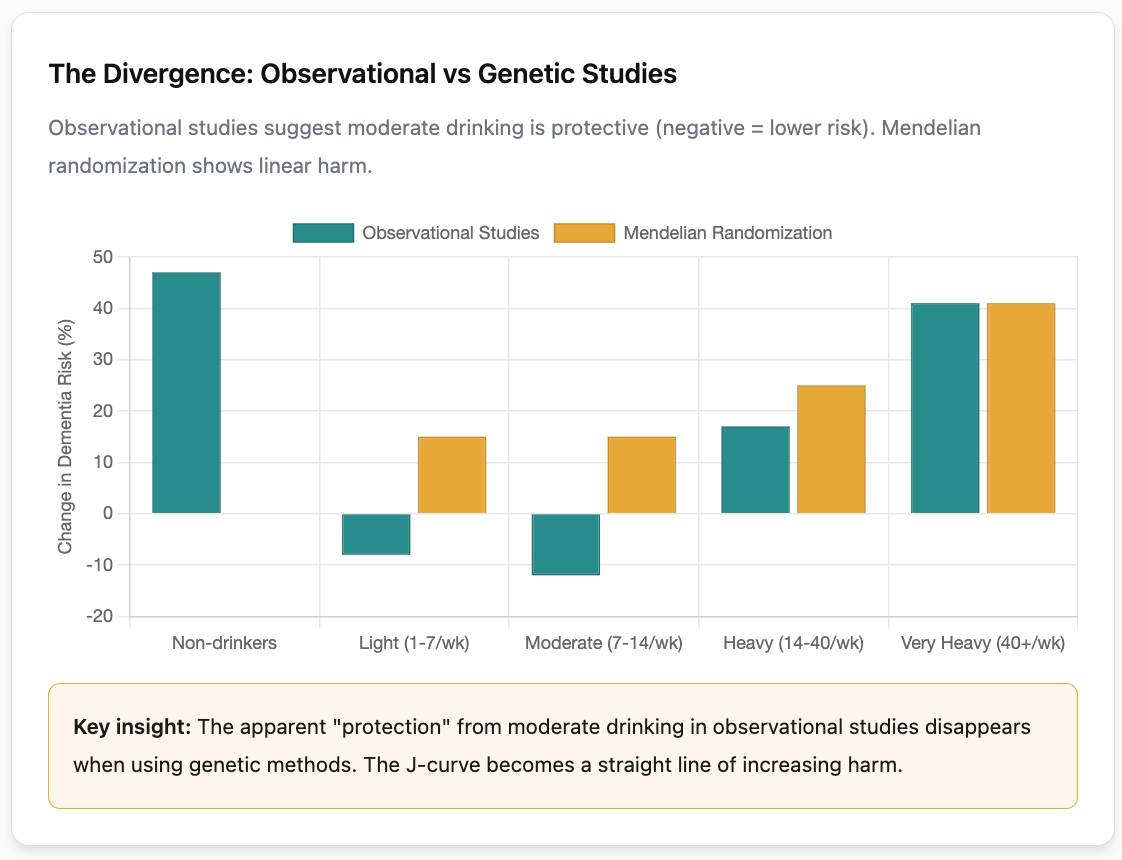
What observational studies show (likely confounded): In the 2025 Topiwala et al. study, conventional observational analysis found that compared to light drinkers (fewer than 7 drinks per week), moderate drinkers (7 to 14 drinks per week) in the UK Biobank actually had lower dementia incidence. Heavy drinkers (more than 40 drinks per week) had 41% higher risk (HR 1.41, 95% CI 1.15 to 1.74), and those with alcohol dependence had 51% higher risk (HR 1.51, 95% CI 1.42 to 1.60).
The Whitehall II Study found that compared to the reference group drinking 1 to 14 units weekly, abstainers had 47% higher dementia risk (HR 1.47, 95% CI 1.15 to 1.89). Among those drinking more than 14 units weekly, each additional 7 units was associated with 17% higher dementia risk.
These observational findings would seem to support moderate drinking. But this is exactly where the MR studies become critical.
What Mendelian randomization studies show (less confounded): The same 2025 study, when analyzed using genetic instruments, found strikingly different results. A one standard deviation increase in genetically predicted alcohol consumption (roughly equivalent to going from 1 to 3 drinks per week, or from 5 to 16 drinks per week) was associated with 15% higher dementia risk (OR 1.15, 95% CI 1.03 to 1.27). Participants averaging 12 drinks per week showed 9% higher dementia risk (OR 1.09, 95% CI 1.04 to 1.15). A twofold increase in genetic liability for alcohol use disorder was associated with 16% higher dementia risk (OR 1.16, 95% CI 1.03 to 1.30).
Crucially, the genetic analyses showed no U-shaped curve. Risk increased monotonically from the lowest consumption levels measured.
How large are these effects?
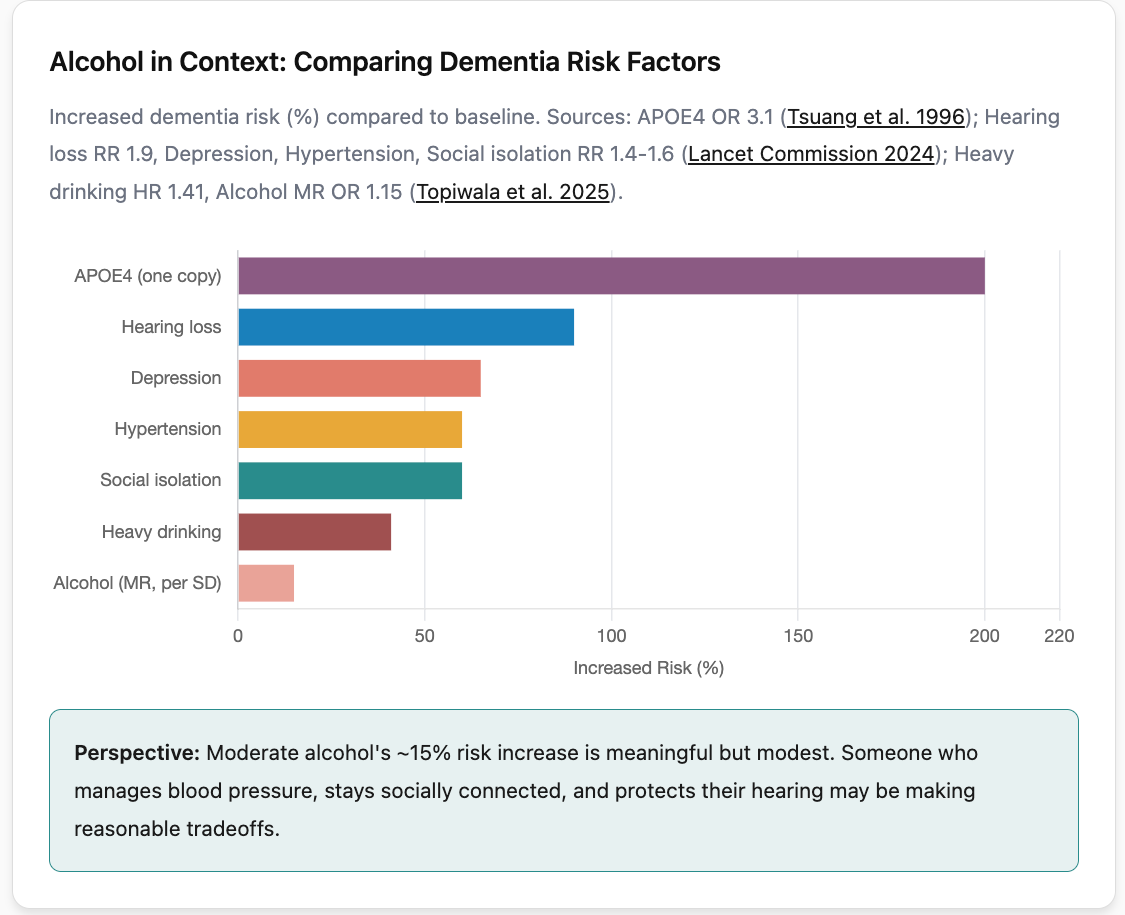
To put the MR-derived 15% increase per roughly 2 to 10 additional drinks weekly in perspective: this is a modest effect size. For comparison, the APOE4 genotype (a single copy) increases Alzheimer’s risk by roughly 3-fold. Depression, hearing loss, and social isolation each increase dementia risk by 50 to 90% according to the Lancet Commission. Hypertension in midlife increases risk by about 60%.
So alcohol’s effect on dementia risk, while real according to MR studies, appears to be smaller than several other modifiable risk factors. This is important context: someone who drinks moderately but exercises regularly, maintains social connections, controls blood pressure, and protects their hearing may be making reasonable tradeoffs. Someone who drinks heavily is facing a more unambiguous risk.
Light drinking (1 to 7 drinks per week): Traditional observational studies consistently reported that light drinkers had about 8% lower dementia risk compared to non-drinkers. However, when Mendelian randomization studies removed confounding factors, this protective effect vanished. The 2025 Oxford/Yale study found that even 1 to 3 drinks per week was associated with 15% higher dementia risk when analyzed using genetic methods. That said, the confidence intervals at very low consumption levels are wider, and some researchers argue we cannot definitively rule out a threshold below which effects are negligible.
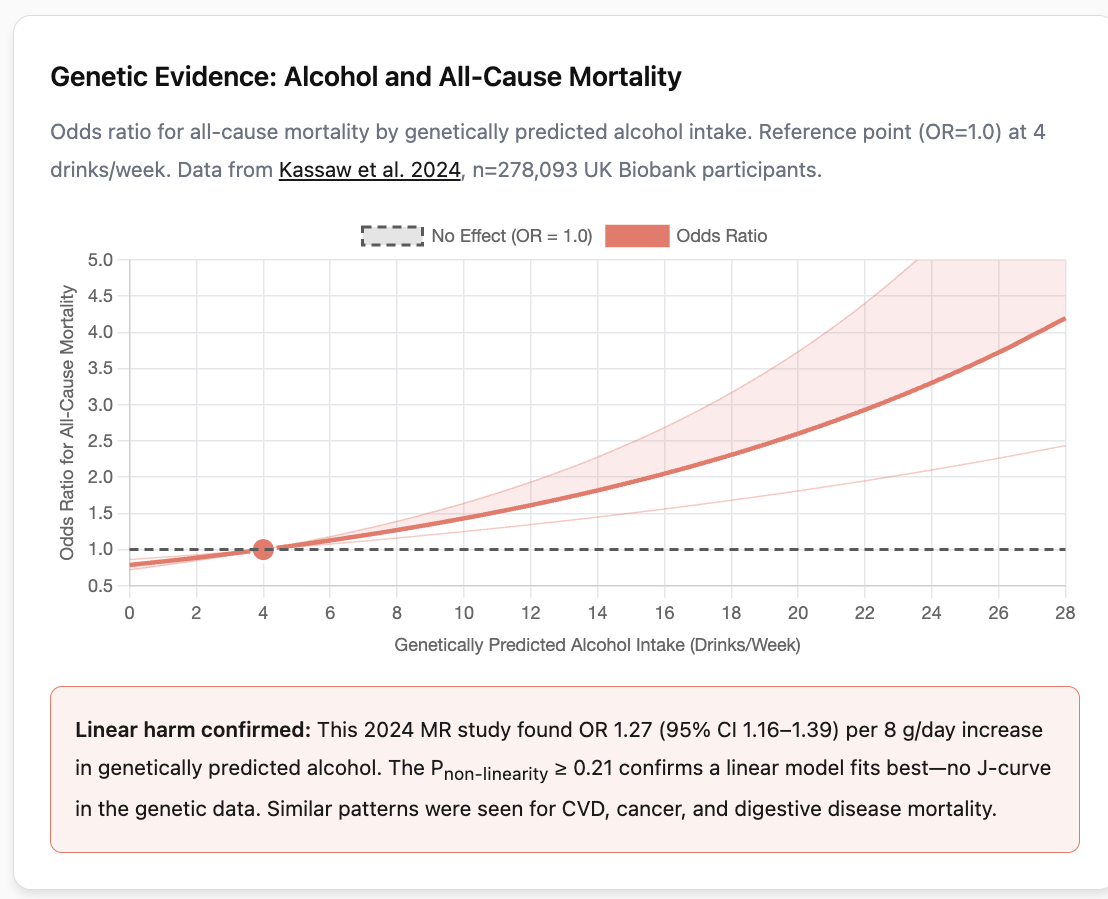
Moderate drinking (7 to 14 drinks per week): Observational studies often showed the lowest risk in this range. But the largest Mendelian randomization studies reveal a linear dose-response, as consumption increases, so does risk, with no plateau or sweet spot in the moderate range. The 2024 UK Biobank MR study explicitly tested for non-linearity and found no evidence of a J-shaped curve in the genetic data.
Heavy drinking (14+ drinks per week): All research methods agree that heavy drinking dramatically increases dementia risk. A 2018 Lancet Public Health analysis of over 1 million French hospital admissions found that alcohol use disorders more than tripled dementia risk, making excessive alcohol the strongest modifiable risk factor identified. Among people who developed dementia before age 65, nearly 40% had alcohol-related diagnoses.
Binge drinking: The pattern of drinking matters, not just the total amount. The Finnish Twin Study found that binge drinking (five or more drinks in a session) monthly increased dementia risk more than threefold, independent of total consumption. Passing out from alcohol twice or more per year was associated with tenfold higher risk.
What brain imaging reveals
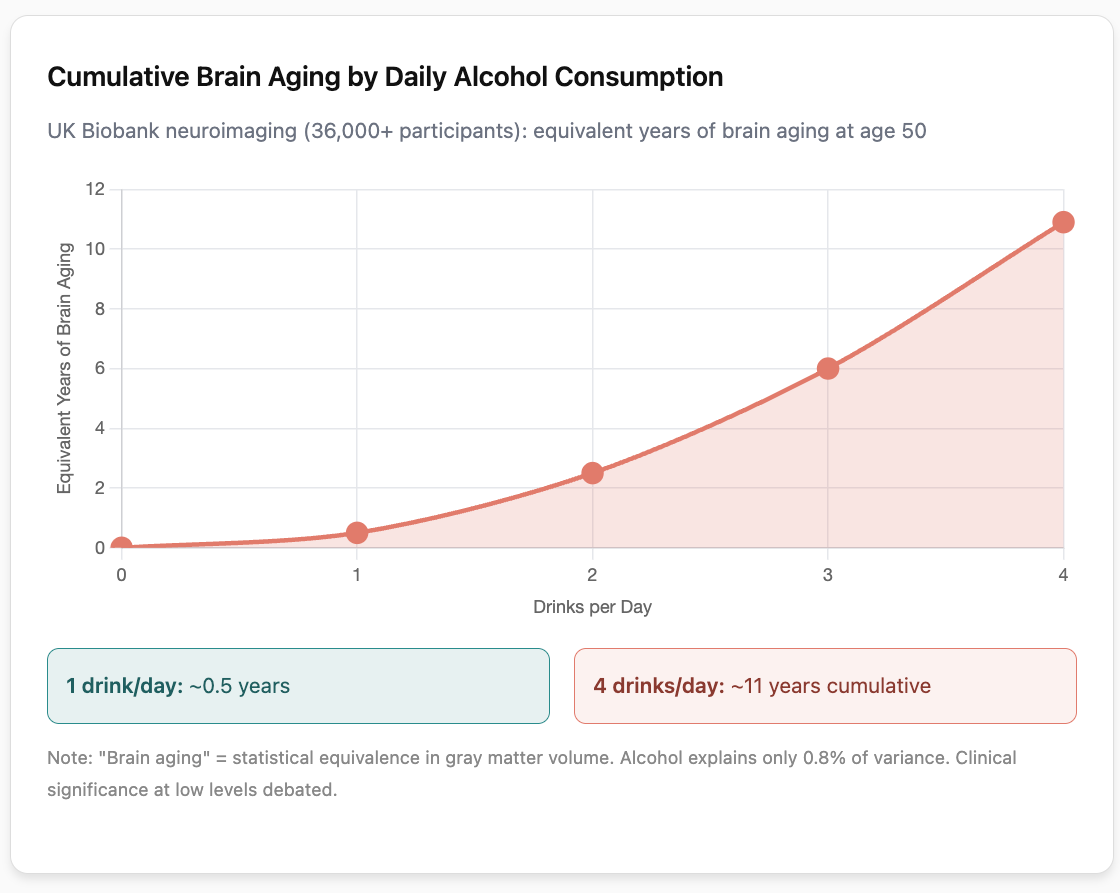
Modern brain scanning studies provide direct evidence of alcohol’s effects on brain structure. A 2022 Nature Communications study examined MRI scans from over 36,000 UK Biobank participants and found measurable brain volume reductions beginning at just 1 to 2 drinks daily.
The relationship was non-linear and accelerated with higher consumption:
- Going from zero to one drink daily: brain aging equivalent to about 0.5 years
- Going from one to two drinks daily: an additional 2 years of brain aging (at age 50)
- Going from two to three drinks daily: an additional 3.5 years of brain aging
- Going from three to four drinks daily: an additional 4.9 years of brain aging
The most affected regions include the frontal cortex (involved in planning and decision-making), the hippocampus (critical for memory), and white matter tracts connecting different brain regions. Heavy drinkers showed frontal cortex volume reductions up to 20%, while four or more drinks daily carried sixfold higher risk of hippocampal shrinkage.
A separate 2022 PLOS Medicine study found that alcohol consumption above 7 drinks per week was associated with higher iron deposits in the basal ganglia, a potential mechanism for cognitive decline.
A note of caution about interpreting these numbers: These imaging studies are observational and subject to some of the same confounding concerns as other observational research, though they do provide more objective measurements than self-reported cognitive outcomes. The effect sizes are also relatively small in absolute terms: alcohol explained about 0.8% of variance in gray matter volume, which is statistically significant in large samples but leaves over 99% of the variation explained by other factors.
How alcohol damages the brain
Several mechanisms explain how alcohol harms brain health:
Direct toxicity: When the body metabolizes alcohol, it produces acetaldehyde and reactive oxygen species that damage cell membranes and proteins. This oxidative stress is particularly harmful to brain cells. The toxic byproduct 4-hydroxynonenal increases up to 40% in affected tissue.
Inflammation: Alcohol triggers brain immune cells (microglia) to produce inflammatory signals including TNF-alpha, IL-1beta, and IL-6. Even single binge episodes prime these cells, making subsequent exposures cause greater inflammatory responses. Chronic low-grade neuroinflammation is increasingly recognized as a driver of neurodegeneration.
Thiamine deficiency: Up to 80% of people with severe alcohol use disorder have thiamine (vitamin B1) deficiency, which can cause Wernicke-Korsakoff syndrome. This condition damages the mammillary bodies, thalamus, and hippocampus, and 80% of cases go undiagnosed until autopsy. Fortunately, supplementing vitamin B1 is an easy and cheap solution.
Vascular effects: Alcohol raises blood pressure and can damage blood vessels, reducing blood flow to the brain over time.
Iron accumulation: Moderate alcohol consumption is associated with increased iron deposition in brain regions, which may contribute to oxidative damage.
Why earlier research found the opposite
Understanding why decades of research suggested moderate drinking was protective helps explain why the new findings are more reliable. Several systematic biases affected observational studies:
The “sick quitter” effect: When people become ill, they often stop drinking on doctors’ orders or because they feel too unwell. Studies that classify these former drinkers as “abstainers” make the non-drinking group appear less healthy than it actually is. A 2016 meta-analysis found that when studies properly accounted for this, the protective effect of moderate drinking disappeared.
Healthy user bias: Researchers comparing abstainers to moderate drinkers on 30 health risk factors found that abstainers had elevated risk on 27 of them, including obesity, exercise patterns, diet quality, and income. Moderate drinkers are simply healthier on average for reasons unrelated to their drinking.
Social engagement confounding: As discussed above, moderate drinkers tend to be more socially connected, and social connection itself protects brain health. Studies rarely controlled adequately for social network size, frequency of social activities, or quality of relationships.
Survivor bias: Most alcohol-related deaths occur before age 50, but most dementia studies recruit participants after that age. People who drank heavily but died young from accidents, liver disease, or other causes are not present in older cohorts. The “healthy moderate drinkers” who remain may simply be people whose biology allowed them to survive despite alcohol use.
Reverse causation: Dementia develops over 20+ years before diagnosis. People in the early stages often reduce their drinking due to subtle cognitive changes, caregiver recommendations, or medication interactions. This makes it appear that non-drinking predicts dementia when actually early dementia predicts non-drinking.
Measurement problems: People consistently underreport their drinking by 40 to 60%. Light drinkers in surveys may actually be moderate drinkers, and moderate drinkers may actually be heavy drinkers, distorting the apparent dose-response relationships.
Genetic vulnerability: APOE4 and alcohol
The APOE4 gene variant, carried by about 25% of the population and associated with higher Alzheimer’s risk, may interact with alcohol effects. Several prospective studies have examined this gene-environment interaction, though findings are not entirely consistent.
A landmark 2004 Finnish study (Anttila et al., BMJ) followed 1,018 adults for 23 years from midlife to old age and found a striking interaction: among APOE4 carriers, frequent drinkers had an odds ratio of 3.6 for dementia compared to non-carriers who never drank, while infrequent drinkers had an OR of 2.3. The interaction was statistically significant (P=0.04). Crucially, non-carriers showed similar dementia odds regardless of alcohol consumption, suggesting the risk amplification is specific to APOE4 carriers. This was a prospective population-based study, though limited by its modest sample size and reliance on self-reported drinking frequency rather than quantity.
Similarly, a 2000 French study (Dufouil et al., Epidemiology) of 1,389 adults aged 59-71 with 4-year follow-up found that drinking was associated with decreased risk of cognitive deterioration in non-APOE4 carriers, but the opposite association in APOE4 carriers. Later work from the Framingham Heart Study (Downer et al., 2014) found that light-to-moderate alcohol consumption during late life was associated with greater decline in learning and memory among APOE4 carriers, while potentially protective among non-carriers.
However, not all studies replicate this interaction. A 2022 study of the Honolulu-Asia Aging Study (n=2,416 Japanese-American men, nearly 40-year follow-up) found that while heavy drinking increased cognitive impairment risk overall (HR 1.36-1.46), the APOE4 interaction did not reach statistical significance, possibly due to limited power in subgroup analyses. The biological explanation for an interaction, when present, may involve APOE4’s reduced efficiency at clearing amyloid-beta proteins combined with alcohol-induced oxidative stress creating a compounding effect.
What this means practically: If you carry an APOE4 allele (which can be determined through genetic testing), there is suggestive but not definitive evidence that you may be more vulnerable to alcohol’s cognitive effects than non-carriers. The effect sizes in positive studies are substantial (2-4 fold increased dementia risk for drinking APOE4 carriers), but the evidence base consists of modest-sized observational studies rather than large-scale MR analyses. For APOE4 carriers concerned about brain health, this uncertainty argues for greater caution with alcohol consumption, even at moderate levels.
Does the type of alcohol matter?
Wine, particularly red wine, has long been considered the “healthiest” alcoholic beverage. A 2022 UK Biobank analysis of over 350,000 people found that wine drinkers showed a U-shaped risk curve with lowest dementia rates at about 2 glasses daily, while beer and spirits showed purely dose-dependent increases in risk.
The resveratrol hypothesis offers a biological explanation: red wine contains this antioxidant compound, which has shown neuroprotective effects in laboratory studies. However, the math does not support drinking wine for resveratrol. A glass of red wine contains about 200 micrograms of resveratrol, while clinical trials showing cognitive benefits use 500 to 2,000 milligrams, equivalent to drinking roughly 20 bottles of wine daily according to the Alzheimer’s Drug Discovery Foundation.
The more likely explanation for wine’s better profile in observational studies lies in who drinks wine and how. Wine drinkers tend to have higher income, better education, greater healthcare access, and healthier overall lifestyles. They are more likely to follow Mediterranean dietary patterns and to drink with meals (which slows alcohol absorption). When the 2025 Mendelian randomization study controlled for these factors using genetics, no beverage showed protective effects.
Can the brain recover?
The good news is that brain volume begins recovering within weeks of stopping drinking. A study using serial MRI scans found that gray matter starts regenerating within the first two weeks of abstinence, with the fastest recovery in the first month. By about 7 months of abstinence, significant recovery was visible in 26 of 34 brain regions examined.
However, recovery is not guaranteed and depends on several factors: duration and severity of prior drinking, presence of other health conditions like hypertension or diabetes, smoking history, and age. Memory deficits from Wernicke-Korsakoff syndrome resolve fully in only about 25% of cases.
Beyond the brain: alcohol and cancer risk
While this article focuses on brain health, any complete assessment of alcohol’s risks must address cancer. In January 2025, the U.S. Surgeon General recommended that alcoholic beverages carry cancer warning labels, similar to cigarettes. This recommendation reflects decades of accumulating evidence.
What observational studies show: The International Agency for Research on Cancer classifies alcohol as a Group 1 carcinogen (the highest certainty category). Observational studies have linked alcohol to cancers of the mouth, throat, larynx, esophagus, liver, colon, rectum, and female breast. The World Health Organizationestimates that 4.1% of all new cancer cases globally in 2020 were attributable to alcohol.
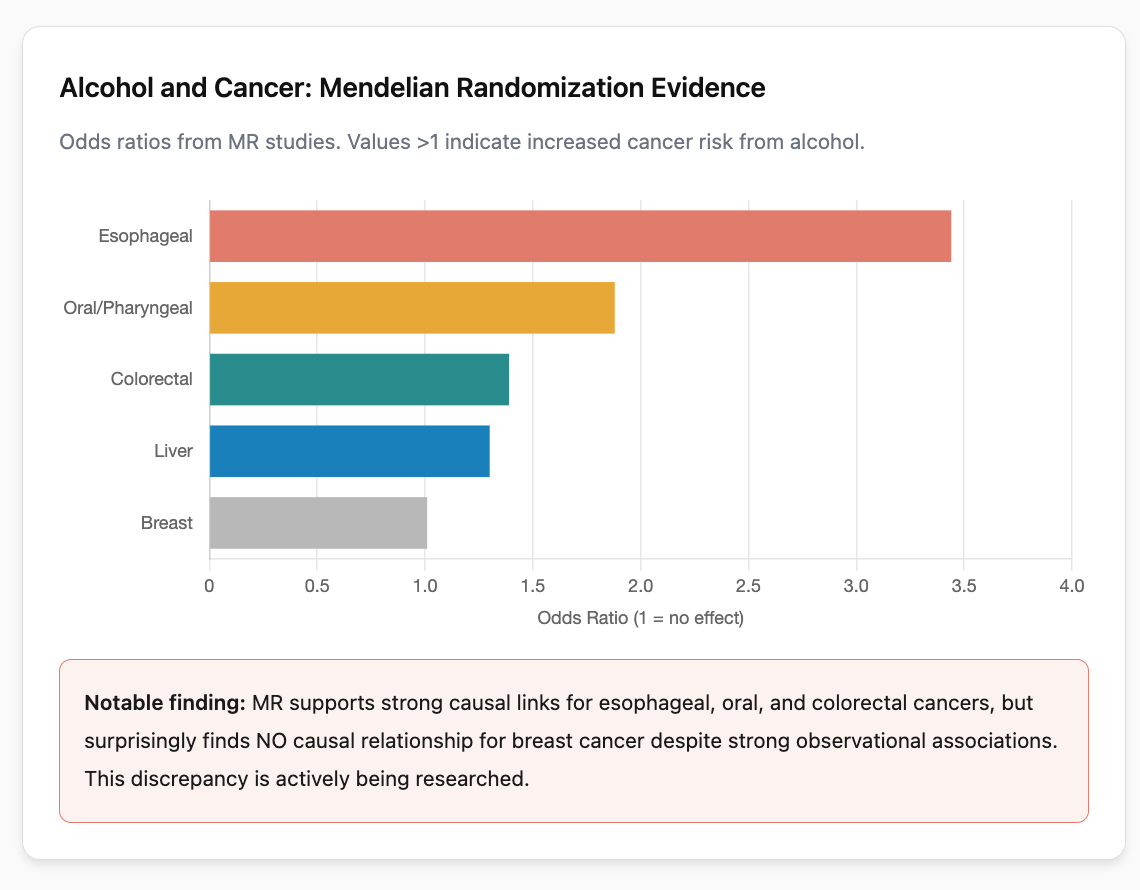
What Mendelian randomization adds: A 2024 systematic review of 70 MR studies found significant causal associations between alcohol and several cancers. The strongest MR evidence supports causal relationships for:
- Esophageal cancer: OR 3.44 (95% CI 1.19 to 9.89) after removing outlier variants
- Colorectal cancer: OR 1.39 (95% CI 1.27 to 1.52) per drink per week in Asian populations; OR 1.08 (95% CI 1.05 to 1.12) for ever vs. never drinkers
- Head and neck cancers: Multiple MR studies support causality, with one finding OR 1.88 for oral/oropharyngeal cancer
- Liver cancer (hepatocellular carcinoma): Supported by MR evidence, consistent with alcohol’s known hepatotoxicity
Where MR evidence is weaker: Interestingly, MR studies have not consistently supported a causal relationship between alcohol and breast cancer, despite strong observational associations. A 2020 MR study using data from 1.5 million individuals found no compelling evidence for causality (OR 1.01, 95% CI 0.85 to 1.21). This discrepancy remains unexplained and is an active area of research. It may reflect limitations of current genetic instruments, differences in relevant exposure windows, or true biological differences in how alcohol affects different cancer types.
What do these numbers mean in absolute terms? Odds ratios can be misleading without context. The table below translates MR findings into absolute risk using SEER baseline cancer incidence data:
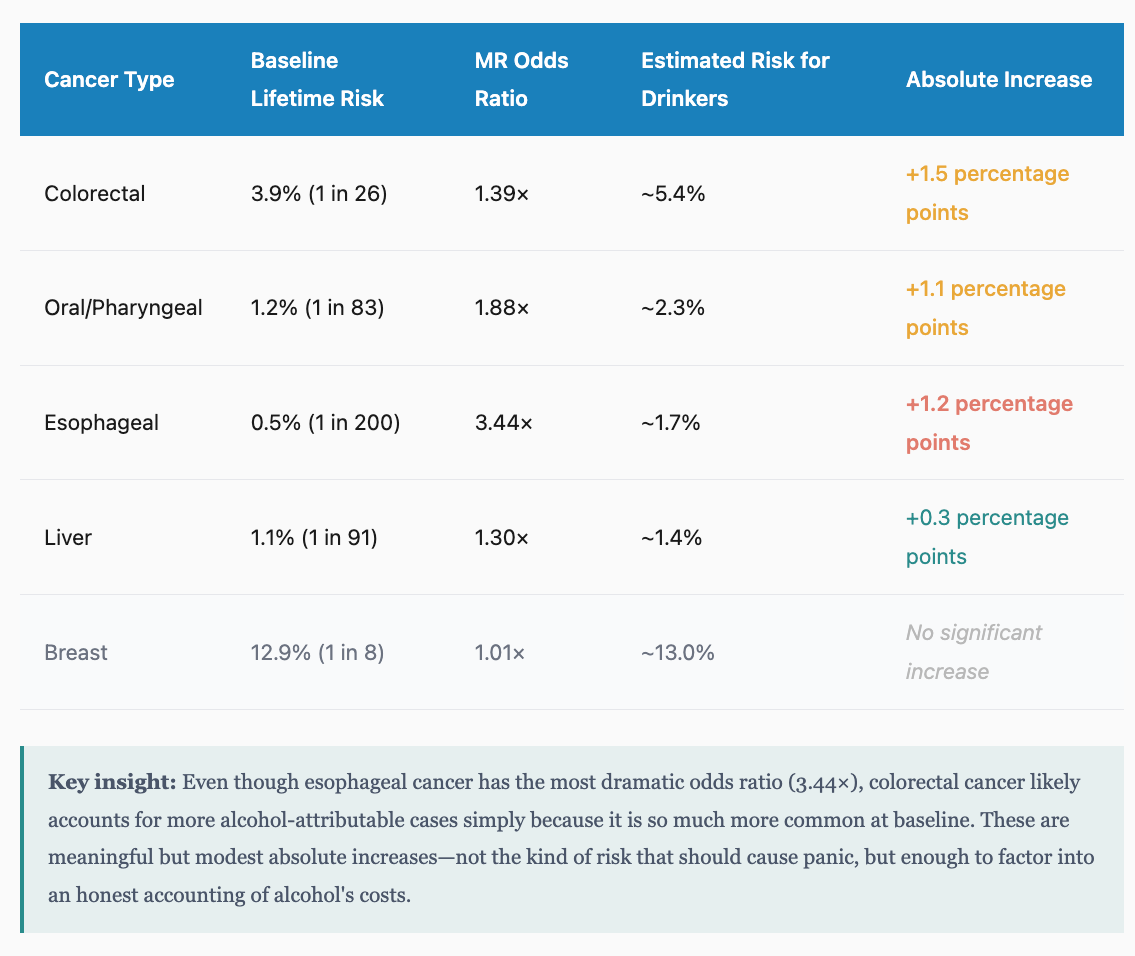
The mechanism: Alcohol’s carcinogenic effects operate through multiple pathways. Acetaldehyde, the first metabolite of alcohol breakdown, is itself a carcinogen that damages DNA. Alcohol also generates reactive oxygen species, interferes with nutrient absorption (particularly folate), affects hormone levels, and may act as a solvent that helps other carcinogens penetrate tissues.
No safe threshold: Unlike the ambiguity around dementia at very low consumption levels, the cancer evidence suggests risk increases from the first drink. A 2018 Global Burden of Disease analysis concluded that the level of alcohol consumption that minimizes health loss is zero.
This cancer evidence strengthens the case for caution about alcohol consumption, even when the brain-specific evidence at low doses remains somewhat uncertain.
The social connection confound: why moderate drinkers may seem healthier
One of the most important and often overlooked factors explaining the apparent health benefits of moderate drinking is social connection. Moderate drinkers are not just consuming alcohol; they are often participating in social rituals that themselves have powerful health benefits.
Consider how moderate drinking typically occurs: wine with dinner alongside family or friends, a beer at a pub with colleagues, champagne at celebrations. These are fundamentally social activities. The 2020 Lancet Commission on Dementia identified social isolation as an independent risk factor for dementia, estimating it accounts for about 4% of dementia cases worldwide. Multiple studies have shown that loneliness and social isolation accelerate cognitive decline as much as or more than many physical health factors.
When observational studies compare moderate drinkers to non-drinkers, they are often unknowingly comparing socially engaged people to a mixed group that includes both socially connected abstainers and isolated individuals who avoid social situations (including those where alcohol is served). Non-drinkers as a group are more likely to be socially isolated, have chronic health conditions that prevent them from socializing, or have cultural or religious backgrounds that limit their social integration in certain communities.
The social context of drinking also affects stress and mental health. Enjoying a drink in a relaxed social setting is quite different physiologically from drinking alone. Social connection reduces cortisol levels, activates the parasympathetic nervous system, and promotes the release of oxytocin, all of which benefit brain health independently of any effect from alcohol.
This creates a classic confounding problem: the apparent benefits of moderate alcohol consumption may actually be benefits of social connection that happen to coincide with drinking. In cultures where moderate drinking is integrated into meals and social gatherings, drinkers receive a double exposure: the harms of alcohol plus the benefits of social engagement. If the social benefits outweigh the alcohol harms at low doses, the net effect looks protective even though alcohol itself is causing damage.
Mendelian randomization studies sidestep this problem because genetic variants affecting alcohol metabolism are (presumed to be) not related to sociability or social network size. When these studies show linear harm from alcohol, it suggests that the apparent protection in observational research was indeed driven by confounding factors like social engagement rather than by alcohol itself.
The real benefits of drinking: what would we lose?
Any honest assessment of alcohol and brain health must grapple with an uncomfortable question: alcohol serves real psychological and social functions that cannot be dismissed as mere addiction or weakness. If public health guidance moves toward recommending abstinence, we need to consider what would need to replace those functions.
Social lubrication and anxiety reduction. Alcohol genuinely reduces social anxiety and lowers inhibitions in ways that facilitate connection. For many people, a drink or two makes conversation easier, reduces self-consciousness, and helps bridge the awkward gaps that can make socializing feel like work. This is not imaginary: alcohol acts on GABA receptors to reduce anxiety, and this pharmacological effect has real social utility. People who are naturally introverted or socially anxious may find that alcohol provides access to social experiences they would otherwise avoid.
Ritual and transition. The end-of-day drink serves as a ritual marker between work and rest. Happy hour, wine with dinner, and nightcaps all signal transitions between modes of being. These rituals provide structure and permission to relax that many people struggle to access otherwise. The act of preparing and consuming a drink creates a pause, a moment of intention, that helps shift mental states.
Shared cultural practice. Drinking together is one of humanity’s oldest bonding rituals, present across virtually every culture. Toasting, buying rounds, sharing bottles: these practices create reciprocity and signal trust. Refusing a drink can still feel like refusing connection in many social contexts, which is why non-drinkers often feel excluded or must actively work to maintain social integration.
Emotional regulation. Many people use alcohol to cope with stress, grief, loneliness, or difficult emotions. While this can obviously become problematic, it is also true that moderate alcohol use provides genuine short-term relief from psychological distress for which many people have no ready substitute.
The substitution problem. If we accept that alcohol causes brain harm and recommend abstinence, we must ask: what fills the void? Non-alcoholic beverages can replicate some rituals but lack the pharmacological effects that reduce anxiety. Meditation and exercise provide stress relief but require effort and discipline. Social activities without alcohol may feel more demanding for those who relied on its lubricating effects. Mental health treatment is often inaccessible, expensive, or stigmatized.
This is not an argument for drinking. It is an argument for honesty about the tradeoffs and for developing realistic alternatives. Public health messaging that simply tells people to stop drinking without addressing the functions alcohol serves is likely to fail or to leave people worse off in other ways. The goal should be helping people access the genuine benefits of social connection, stress relief, and ritual without the neurological costs of alcohol, but achieving that requires acknowledging what alcohol actually provides.
Could other drugs replace alcohol more safely?
If alcohol harms the brain but serves real social and psychological functions, an obvious question arises: are there pharmacological alternatives that could provide similar effects with less neurotoxicity? This question is being actively researched, though no perfect substitute currently exists.
Kava (Piper methysticum): This traditional Pacific Island drink contains kavalactones that act on GABA receptors, producing relaxation and reduced anxiety without the cognitive impairment of alcohol. Kava has been used for centuries in ceremonial and social contexts. Research suggests it has genuine anxiolytic properties, and users report feeling calm and sociable while remaining mentally clear. Unlike alcohol, kava does not appear to cause hangovers or the same pattern of dependence.
However, kava is not without concerns. Reports of liver toxicity emerged in the early 2000s, leading several European countries to temporarily ban it. Subsequent research suggested the liver damage may have been related to non-traditional preparations using stems and leaves rather than roots, or to contaminated products. Traditional water-based preparations of noble kava varieties appear safer, but regulatory oversight is limited and product quality varies. Kava also causes a distinctive skin condition (kava dermopathy) with heavy use and should not be combined with alcohol or other sedatives.
GHB (gamma-hydroxybutyrate): This naturally occurring compound acts on both GHB receptors and GABA-B receptors, producing effects remarkably similar to alcohol: euphoria, sociability, reduced inhibitions, and relaxation. At low doses, users report alcohol-like warmth without the cognitive blunting. GHB is approved medically for narcolepsy (as sodium oxybate/Xyrem) and is used to treat alcohol dependence in Italy and Austria.
The problem with GHB is its extremely narrow therapeutic window. The difference between a dose that produces pleasant effects and one that causes unconsciousness or coma is dangerously small, and this margin varies between individuals and batches. GHB-induced comas appear to cause their own neurotoxicity, with research showing cognitive deficits in users who have experienced multiple overdoses. GHB also produces severe physical dependence with potentially life-threatening withdrawal. While it might theoretically be safer than alcohol if dosing could be precisely controlled, in practice its unpredictability makes it more dangerous for recreational use.
Synthetic GABA modulators (Alcarelle): Professor David Nutt, the former UK government drug advisor, has been developing synthetic compounds designed to mimic alcohol’s pleasant effects while avoiding its harms. His company GABA Labs is working on “Alcarelle,” a partial agonist at specific GABA receptor subtypes.
The key innovations Nutt’s team is pursuing: (1) targeting receptor subtypes that produce relaxation and sociability without sedation, (2) designing partial agonists with a built-in ceiling effect so overdose is impossible, and (3) engineering rapid metabolism so effects wear off predictably. Their botanical product “Sentia” is already available, using plant extracts to modestly enhance GABA activity. The synthetic Alcarelle is expected to be more effective but requires regulatory approval as a novel food ingredient.
This approach is scientifically promising but unproven. No peer-reviewed research on Alcarelle’s effects or safety has been published, and the compounds remain in development. If successful, this could represent a genuine harm-reduction breakthrough, but we are years from knowing whether it delivers on its promise.
Cannabis/THC: Cannabis produces relaxation and mild euphoria through the endocannabinoid system rather than GABA. Some users find it socially lubricating, while others experience increased social anxiety. Unlike alcohol, cannabis does not appear to cause the same pattern of structural brain damage in adults, though heavy use is associated with cognitive effects. Cannabis is not a direct substitute for alcohol’s specific social-facilitating effects, but for some individuals it may serve similar functions with a different risk profile.
What about prescription anxiolytics? Benzodiazepines (Valium, Xanax) work on the same GABA receptors as alcohol and reliably reduce anxiety. However, they carry serious risks: tolerance develops quickly, physical dependence can be severe, and cognitive impairment with chronic use is well-documented. Newer anxiolytics like buspirone lack abuse potential but also lack the acute social effects people seek from alcohol.
It appears that humanity has not yet developed a pharmacological tool that provides alcohol’s social benefits without significant risks. This doesn’t mean such a tool is impossible, just that we haven’t created it yet. In the meantime, the most evidence-based approaches remain: reducing alcohol consumption, maintaining the social practices that make drinking meaningful, and being honest about the tradeoffs involved in any substance use.
What the evidence means in practice
The World Health Organization stated in 2023 that “when it comes to alcohol consumption, there is no safe amount that does not affect health.” Canada’s 2023 guidelines reduced the low-risk threshold from 15 drinks weekly for men to just 2 drinks per week for everyone. The 2024 Lancet Commission on Dementia now lists excessive alcohol as an established modifiable risk factor.
The contrast with previous understanding is stark. As recently as 2015, the J-curve was the dominant paradigm, moderate drinking was considered cardioprotective, and brain effects were primarily studied only in heavy drinkers. The convergence of Mendelian randomization methods, large-scale brain imaging studies, and systematic bias analyses has fundamentally changed the scientific consensus.
The bottom line
Several key advances have reshaped our understanding of alcohol and brain health:
On causation: Mendelian randomization has provided tools to separate correlation from causation. The largest and most recent studies (2024-2025, n > 2 million) reveal linear relationships between alcohol consumption and increased dementia risk, with no evidence of protection at any level. Earlier MR studies (2020) found null associations, but the newer studies are substantially larger and use more sophisticated genetic instruments.
On brain structure: Large-scale brain imaging (36,000+ participants) has demonstrated detectable brain shrinkage at consumption levels of just 1 to 2 drinks daily, with non-linear acceleration of harm at higher levels. However, effect sizes are modest—alcohol explains less than 1% of variance in brain volume—and the clinical significance at low-moderate levels remains uncertain.
On cancer: MR studies provide strong evidence for causal links between alcohol and esophageal (OR 3.44), oral/pharyngeal (OR 1.88), colorectal (OR 1.39), and liver cancer (OR 1.30). However, absolute risk increases are modest: even esophageal cancer, with the highest odds ratio, rises from a 0.5% baseline to roughly 1.7% lifetime risk. Surprisingly, MR finds no causal relationship for breast cancer despite strong observational associations.
On genetic vulnerability: Several prospective studies suggest APOE4 carriers may face amplified risk from alcohol, with odds ratios of 2-4 for dementia among drinking carriers compared to non-drinking non-carriers. However, not all studies replicate this interaction, and the evidence base consists of modest-sized observational cohorts rather than large MR analyses.
On methodology: Systematic analyses have identified specific biases, sick quitter effect, healthy user bias, social engagement confounding, survivor bias, that generated apparent protective effects in earlier observational research. Population stratification (particularly the Asian flush variant) and pleiotropy remains a concern, though large studies address this by restricting to single ancestries and using multiple different polygenic scores.
On what we’d lose: Alcohol provides genuine neurological effects that facilitate social bonding: GABA-mediated anxiety reduction, dopamine-driven reward, and dampened self-monitoring. No currently available alternative matches this combination of rapid onset, reliable effects, cultural integration, and legal availability. Kava, GHB, and experimental compounds like Alcarelle each have significant limitations.
What to do with this information
The science has clearly moved away from recommending moderate drinking for brain health. The question is what to recommend instead, and here honest answers become harder.
For those who don’t drink or drink very little: There is no evidence to suggest starting. The old advice that a glass of wine might help your brain is no longer supported by the evidence.
For those who drink moderately and enjoy it: The decision is genuinely uncertain. The brain imaging studies suggest detectable effects at 1 to 2 drinks daily, but effect sizes are small and the clinical significance at low levels is unclear. The absolute cancer risk increases are meaningful but modest, on the order of 1-2 percentage points for most cancers. Someone who drinks a glass of wine with dinner in a social context is receiving both a potential harm (the alcohol) and a potential benefit (the social connection, the ritual, the stress transition). Whether the net effect is positive or negative may depend on individual factors we cannot easily measure.
For APOE4 carriers: If you know you carry one or more APOE4 alleles, there is suggestive evidence that you may be more vulnerable to alcohol’s cognitive effects. The effect sizes in positive studies are substantial (2-4 fold increased dementia risk), though the evidence comes from modest-sized observational studies. For APOE4 carriers concerned about brain health, this uncertainty argues for greater caution, even at moderate levels.
For those who drink heavily: The evidence is unambiguous. Heavy alcohol consumption damages the brain, and reducing intake will likely improve brain health outcomes. The good news is that brain volume begins recovering within weeks of stopping, with significant recovery visible by 7 months of abstinence.
For everyone: If you do decide to reduce or eliminate alcohol, do not let go of the social practices that surrounded it. Find other ways to mark transitions, other shared rituals, other contexts for connection. The research suggests that social engagement itself protects brain health—the Lancet Commission estimates social isolation accounts for 4% of dementia cases. The worst outcome would be trading alcohol for isolation.
No MR study has found that alcohol protects brain health. The most rigorous recent evidence suggests linear harm beginning at low consumption levels. But multiple sources of uncertainty remain: MR’s pleiotropy problem means the harm attributed to alcohol may partly reflect correlated traits like impulsivity; the effect sizes at moderate consumption are modest; the absolute risks are not catastrophic; and the social and psychological functions alcohol serves are real. Without randomized trials, which may never be ethically feasible, we are triangulating from imperfect methods. For most moderate drinkers, this is not an emergency requiring immediate action, it’s information to factor into ongoing decisions about health tradeoffs, with appropriate humility about what we actually know.